121 - Weaning guidelines for Stopping CPAP in Preterm Infants Born at ≤29 Weeks Estimated Gestational Age: A QI initiative
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4119.121
Khawar Nawaz, University of Texas Southwestern Medical School, Dallas, Texas, TX, United States; Venkatakrishna Kakkilaya, UT Southwestern Medical Center, Dallas, TX, United States; sheron A.. Wagner, Baylor University School of Nursing, Telephone, TX, United States; Michael Price, Children's Mercy Hospitals and Clinics, Kansas City, MO, United States; Annesha Dutta, University of Texas Southwestern Medical School, Dallas, TX, United States
Fellow University of Texas-Southwestern Medical Center Dallas, Texas, United States
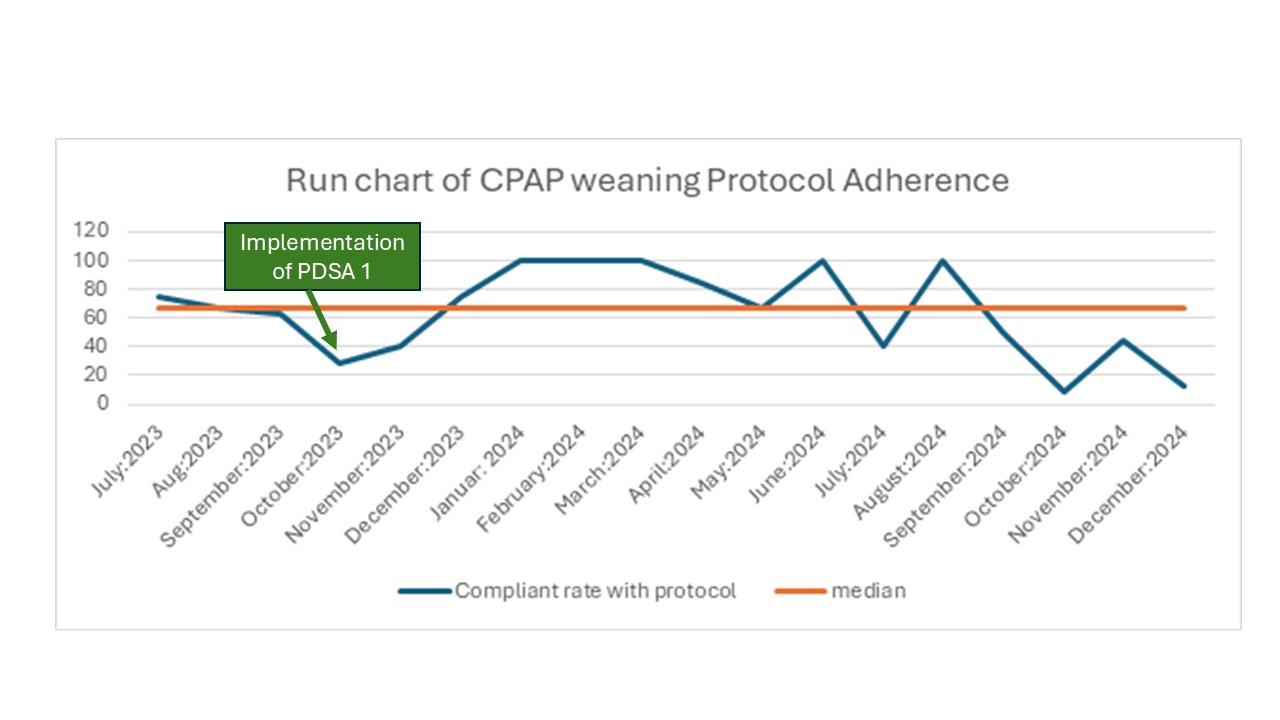
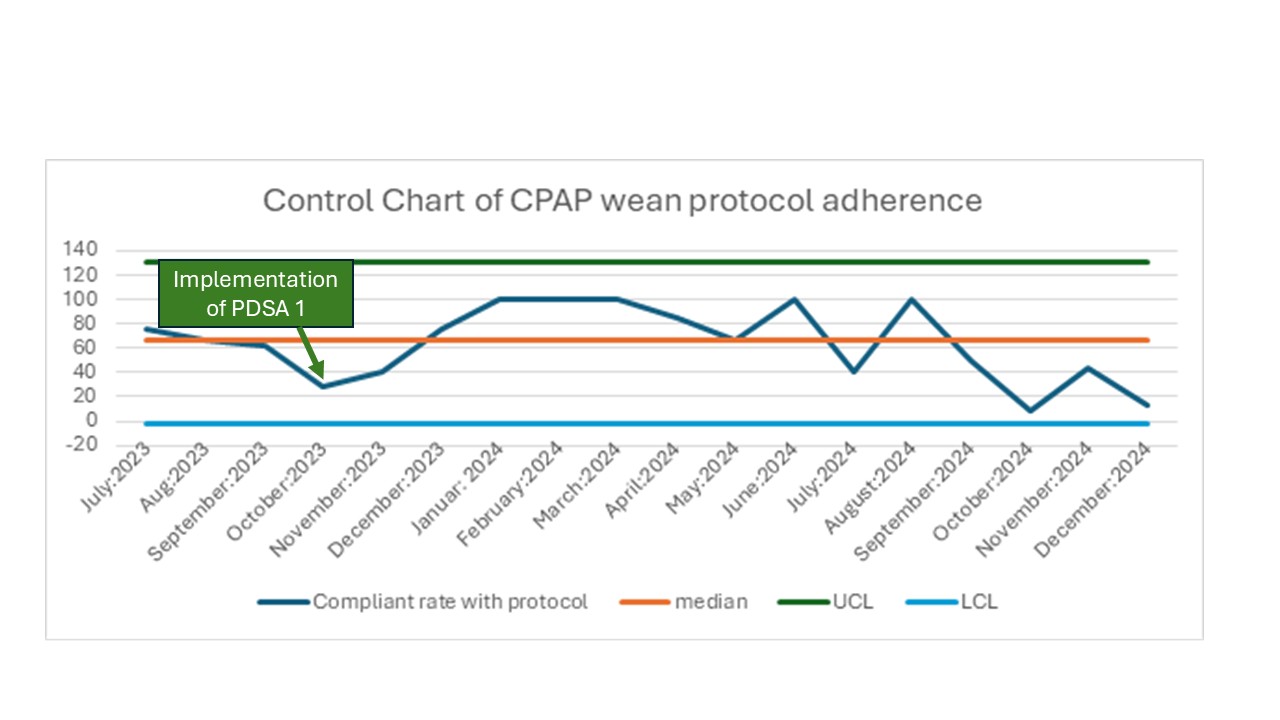
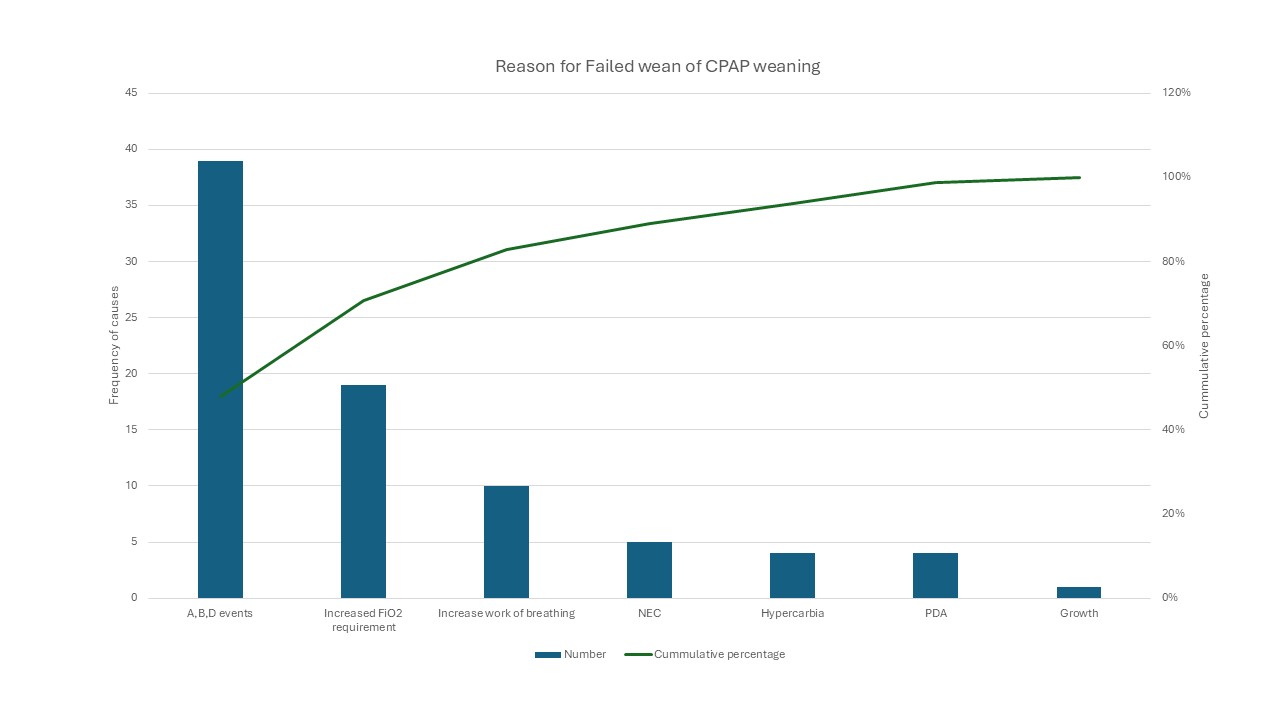
Background: Continuous Positive Airway Pressure (CPAP) is a cornerstone of respiratory support for preterm neonates. However, optimal strategies for CPAP weaning remain unstandardized, leading to variable practices across NICUs. Standardizing CPAP weaning using a structured protocol may reduce variation and improve clinical efficiency. Objective: To improve adherence to a CPAP weaning protocol in preterm infants < 29 weeks gestation born at parkland hospital between July 2023-to December 2024 from a baseline of < 50% to >80% by end of the study period. Design/Methods: A multidisciplinary NICU team at Parkland Hospital initiated a quality improvement (QI) project from July 2023- December 2024 using Plan-Do-Study-Act (PDSA) cycles. Interventions included Provider education, bedside visual aids and quarterly feedback session on adherence. Data were collected monthly from the electronic medical record. Run and control charts were used to analyze trends and special cause variation. A Pareto chart identified reason for failure of CPAP weaning. Results: Among 185 eligible infants during the study duration, 133 remained in the unit for the study duration. Over 14 months, adherence rates demonstrated variability with an overall median of 65%. Improvement was observed during early 2024, reaching 100% after targeted education and feedback to the teams involved in taking care of neonates in Unit. But rates declined later in the year, Figure 1. The control chart revealed all points within control limits, suggesting common cause variation rather than sustained process change ,Figure 2. About half of the eligible neonates failed the protocol weans. Pareto analysis showed that Apnea, Bradycardia, and Desaturation and increase FiO2 requirements were main causes of failed weaning, Figure 3. While provider deviation from protocol and clinical judgement overrides were the main contributor of non-adherence to CPAP weaning protocol.
Conclusion(s): Implementation of standardized CPAP weaning protocol improved adherence transiently but did not achieve sustained control. Continuous provider engagement, reinforcement of education, and integration of EMR-based reminders are essential for maintaining adherence. Future PDSA cycles will focus on real-time feedback and process automation to achieve durable improvement and more consistent respiratory care practices for preterm infants.
Figure 1: Run Chart of CPAP weaning Protocol
Figure 2: Control chart of CPAP weaning Protocol
Figure 3: Pareto chart on causes of failed weaning

 Credit")
 photo")