MD, PhD Kumamoto City Hospital Kumamoto, Kumamoto, Japan
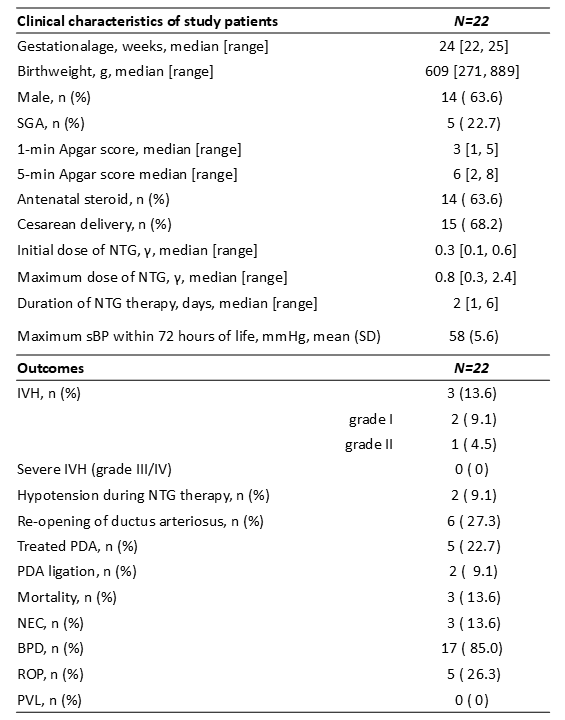
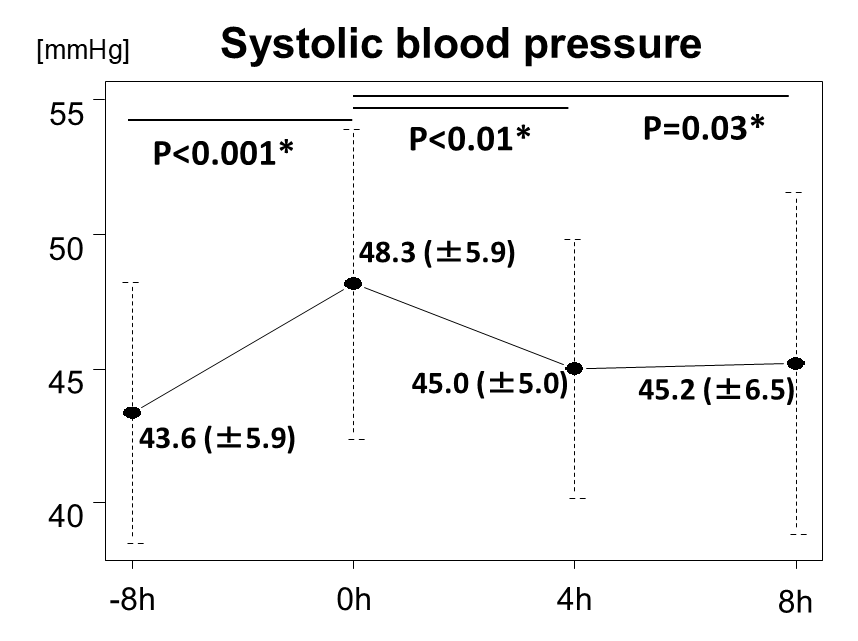
Background: Severe intraventricular hemorrhage (IVH) remains a major cause of mortality and long-term neurodevelopmental impairment in extremely preterm infants. Increases in systemic blood pressure and cerebral venous pressures have been implicated in the pathogenesis of IVH. Nitroglycerin (NTG), a vasodilator that reduces venous pressure, may therefore have a protective effect against IVH in this population. Objective: To evaluate the efficacy and safety of intravenous NTG for the prevention of severe IVH in extremely preterm infants. Design/Methods: A single-center retrospective chart review was conducted for infants born at < 26 weeks' gestation between January 2019 and December 2024. Intravenous NTG was administered within 72 hours after birth to infants who met all of the following criteria: (1) presence of at least one of the following-systolic blood pressure (sBP) ≥50 mmHg, an sBP rise ≥15 mmHg within 8 hours, or end-systolic wall stress ≥40 g/cm²; (2) adequate sedation; and (3) absence of a hemodynamically significant patent ductus arteriosus. IVH was graded according to Papile's classification using cranial ultrasound performed between 72 and 96 hours of life. Results: Among 104 infants admitted to our NICU during the study period, 22 (21%) received intravenous NTG. The median [interquartile range] gestational age and birth weight were 24 [22-25] weeks and 609 [271-889] g, respectively. The initial NTG dose was 0.3 [0.1-0.6] μg/kg/min, with a treatment duration of 2 [1-6] days. Mean sBP significantly decreased from baseline (0 hours: 48.3 ± 5.9 mmHg) to 4 hours (45.0 ± 5.0 mmHg) and 8 hours (45.2 ± 6.5 mmHg) after NTG initiation (P < 0.05). IVH occurred in 3 infants (13.6%; grade I: 2, grade II: 1), but no cases of severe (grade III or IV) IVH were observed. Two infants (9.1%) developed transient hypotension that resolved after NTG discontinuation without additional intervention. Methemoglobin levels did not differ significantly before and 24 hours after NTG initiation (1.15% vs. 1.24%, P = 0.27). No other major adverse effects related to NTG were identified.
Conclusion(s): Intravenous NTG administration was associated with the absence of severe IVH and no major complications in extremely preterm infants born at 22-25 weeks' gestation. These findings suggest that NTG may have a protective effect against severe IVH, warranting further evaluation in prospective clinical trials.

 photo")