464 - Improving Follow-Up Rates in a High-Risk NICU Clinic: A Quality Improvement (QI) StudyAnalyzing and Targeting the Medical and Social Barriers for Follow-Up
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4455.464
Angella Baby, Cooper Medical School of Rowan University, Sugar Land, TX, United States; Diana Yanni, Cooper Medical School of Rowan University, Philadelphia, PA, United States; Vishwanath Bhat, Cooper University Hospital, Camden, NJ, United States; Vineet Bhandari, The Children's Regional Hospital at Cooper, Camden, NJ, United States; Alla Kushnir, Cooper Medical School of Rowan University, Camden, NJ, United States
Associate Professor of Pediatrics Cooper Medical School of Rowan University Camden, New Jersey, United States
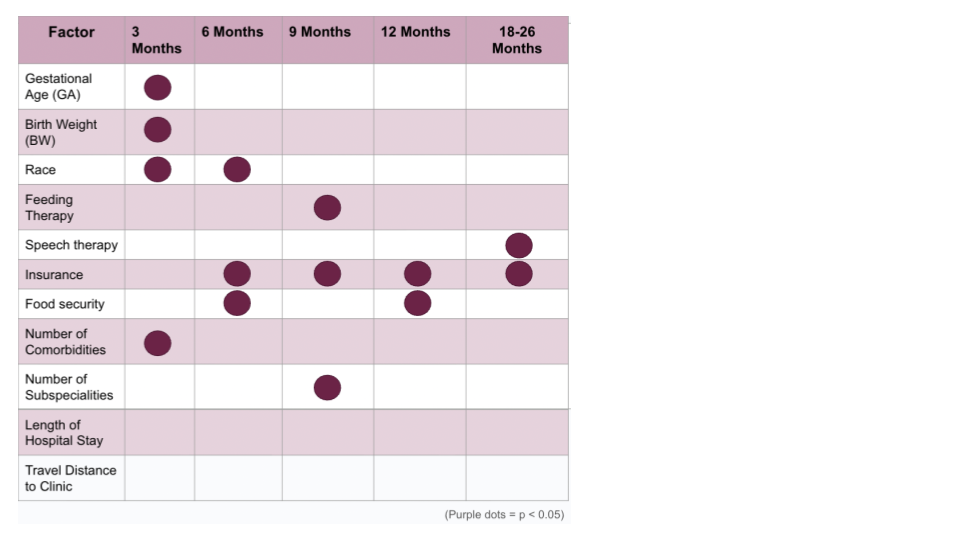
Background: High-risk infant follow-up clinics are vital in monitoring growth and neurodevelopment of infants discharged from the neonatal intensive care unit (NICU). Previous studies report that infants with low clinic attendance rates have increased risk of neurodevelopmental challenges. There may be different medical and social barriers for follow-up in clinics serving a high-risk population. Studying these barriers is essential to improving neurodevelopmental outcomes. The aim of this study is to assess the current follow-up rate in our clinic and to examine the factors related to low attendance. Objective: To assess the current follow-up rate in our clinic and to examine factors that influence this rate. Design/Methods: This study is a retrospective chart review of patients discharged from our level III NICU from January 2020 to December 2021 and scheduled for follow-up at Bright Beginnings, a high-risk follow-up clinic. Demographic maternal and infant data, birth related data, as well as information on neonatal morbidities, measures of neurodevelopment, social factors, and healthcare utilization were collected. Attendance at 3, 6, 9, 12, and 18-26 months corrected age was documented and the rate of follow-up was calculated. Complete follow up was defined as attendance at 5 clinic visits. Results: The rate for complete follow up was 22%. Among 200 patients, 53% identified as White, 32% as African American, 2.5% as Hispanic, 2.5% as Asian, 3.5% as other/mixed. Children with public insurance (68%) were less likely to attend compared to those with private insurance (28%) at the 6, 9, 12, and 18-26 month visits. Patients experiencing food insecurity were less likely to attend the 12 and 18-26 month visits (p= 0.01, p= 0.04). At the 3-month visit, attendance was significantly associated with birth weight (p= 0.004), gestational age (p= 0.01), and increased number of comorbidities (p= 0.04), with lower birth weight and earlier gestational age among those who did not attend. At 3 and 6 months, race (p= 0.03, p= 0.03) was associated with attendance, with lower rates among Black patients. No single factor was significant across all time points, although therapy involvement, food insecurity, and insurance status showed recurrent associations.
Conclusion(s): Attendance at Bright Beginnings clinic is critical in evaluation of health and neurodevelopmental outcomes of high-risk neonates. Early follow-up was primarily influenced by neonatal characteristics, while later follow-up was driven by social factors. The results of this study will be used to design quality improvement interventions to target barriers for attendance.

 photo")