111 - Implementation of an Aortic Arch Watch Protocol for Neonatal Patients at Risk of Coarctation of the Aorta in a Large Tertiary NICU Setting
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4109.111
Grace P. Callahan, Boston Children's Hospital, Watertown, MA, United States; Giulia P. Lima, Boston Children's Hospital, Chestnut Hill, MA, United States; Victoria T. Bradford, Boston Children's Hospital, Boston, MA, United States; Kristin Bonello, Boston Children's Hospital, Boston, MA, United States; Elisabeth Kaza, Brigham and Women's Hospital, CHESTNUT HILL, MA, United States; Alyssa R. Thomas, Brigham and Women's Hospital, SOUTH BOSTON, MA, United States
PGY3 Boston Children's Hospital Watertown, Massachusetts, United States
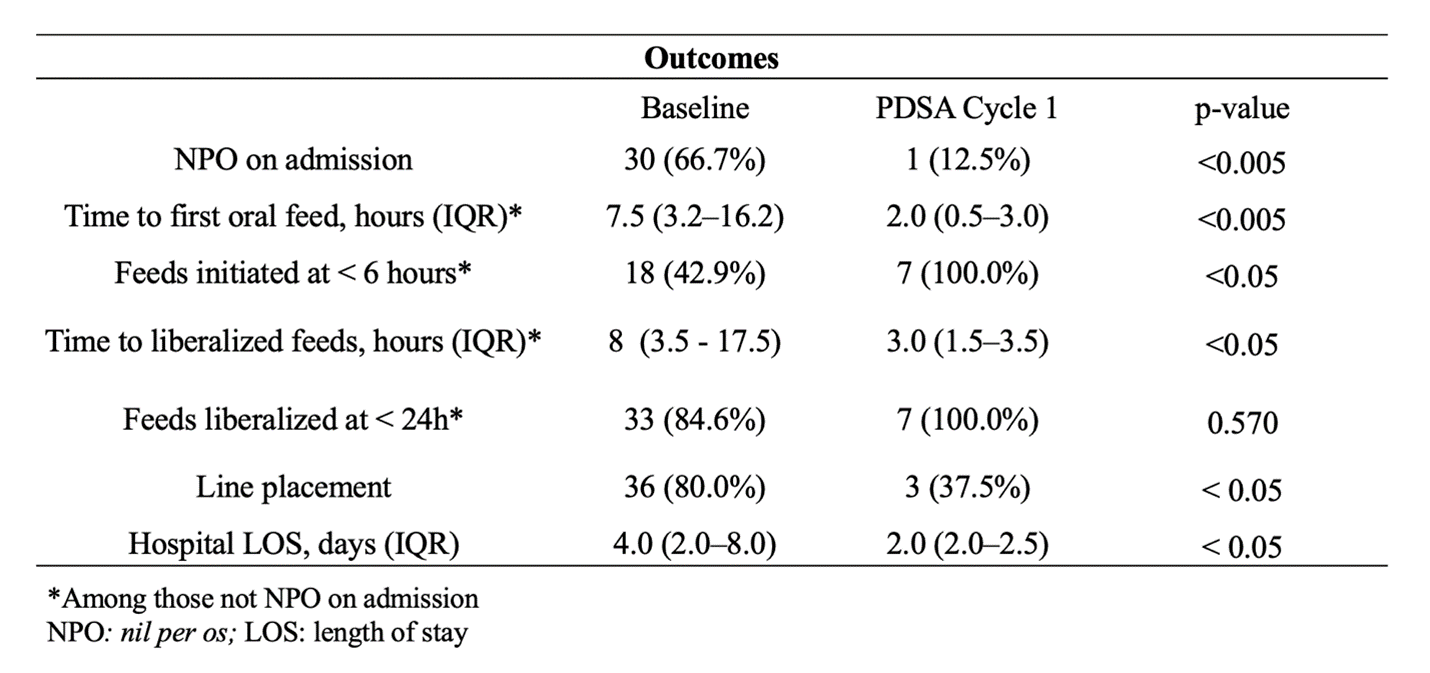
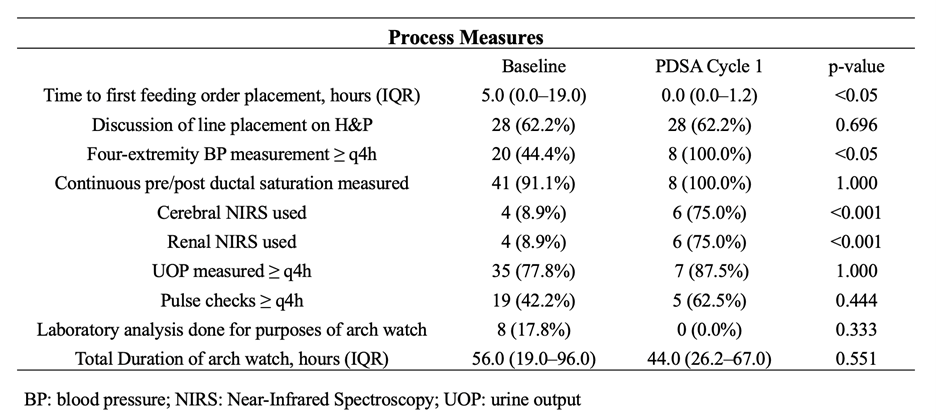
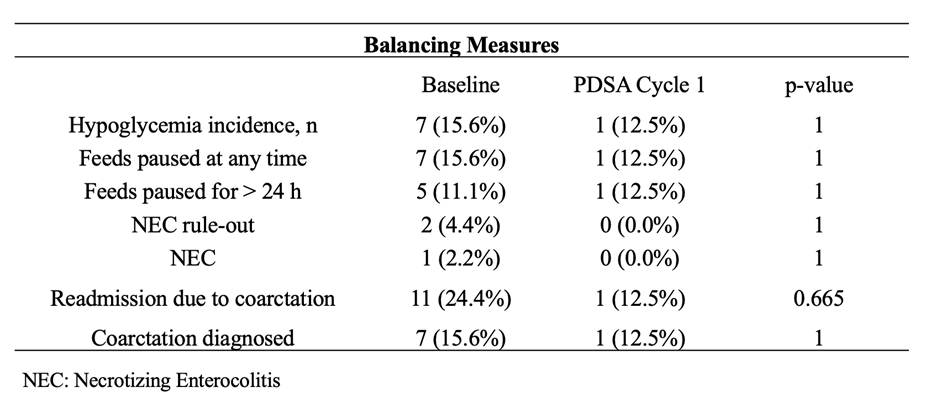
Background: Prenatal suspicion of coarctation of the aorta (CoA) frequently results in postnatal "arch watch" admissions to monitor for evolving arch obstruction with ductus arteriosus closure. Monitoring practices vary widely, and standardizing care has the potential to reduce unnecessary interventions while maintaining patient safety. Objective: To evaluate the impact of a risk-stratified "Arch Watch" clinical practice guideline (CPG) on feeding practices, IV access management, and length of stay among infants admitted for arch watch in a Neonatal Intensive Care Unit (NICU). Design/Methods: We conducted a single-center, pre-post implementation study of infants (>37 weeks gestation) admitted to a level III NICU between October 2020 and August 2025 with low to moderate risk for postnatal CoA based on fetal imaging. The primary aim was to increase the number of infants initiating enteral feeding within the first six hours of life by 30% within one year of protocol implementation. Secondary aims were to reduce intravenous (IV) line placements by 20% and to reduce length of stay by 15%. Balancing measures included feeding intolerance, hypoglycemia, postnatal diagnosis of critical CoA, and unplanned readmission due to CoA. Results: Demographic characteristics were similar between baseline (n=45; 12/2020-10/2024) and post-implementation (n=8; 12/2024-08/2025). The percentage of infants made NPO on admission decreased from 66.7% to 12.5% (p < 0.005). Median time to first oral feed decreased from 7.5 (3.2-16.2) to 2 (0.5-3.0) hours (p < 0.005), infants initiating oral feeds within 6 hours increased from 42.9% to 100% (p < 0.05). IV-line placement decreased from 80.0% to 37.5% (p < 0.05), median hospital LOS decreased from 4 (2.0-8.0) to 2 (2.0-2.5) days (p < 0.05), meeting all predefined improvement targets (Table 1). Process measures showed earlier provider feeding orders and increased standardized perfusion monitoring practices (Table 2). No differences noted in hypoglycemia (15.6% vs 12.5%), feeding interruptions >24h (11.1% vs 12.5%), NEC (2.2% vs 0%), readmission/intervention for CoA (24.4% vs 12.5%), or infants with a true postnatal CoA diagnosis (15.6% vs 12.5%) (Table 3).
Conclusion(s): Implementation of a risk-stratified "arch watch" CPG was associated with significant earlier initiation and advancement of feeds, reduced IV-line placement, and shorter length of stay, without evidence of adverse safety outcomes. Standardizing care for infants with suspected CoA is feasible and may improve resource utilization while maintaining patient safety.
Table 1. Outcomes Between Pre-and Post-Implementation Groups
Table 2. Process Measures Between Pre-and Post-Implementation Groups
Table 3. Balance Measures Between Pre-and Post-Implementation Groups

 Credit")
 photo")