324 - Exploring Parental Experiences of Trauma and Resilience in the NICU: A Qualitative Study of Families of Infants with Hypoxic-Ischemic Encephalopathy
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4318.324
Uchenna Anani, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Jodi Backalar, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Sofia Pauca, Vanderbilt University School of Medicine, Nashville, TN, United States
Associate Professor of Clinical Pediatrics Monroe Carell Jr. Children's Hospital at Vanderbilt Nashville, Tennessee, United States
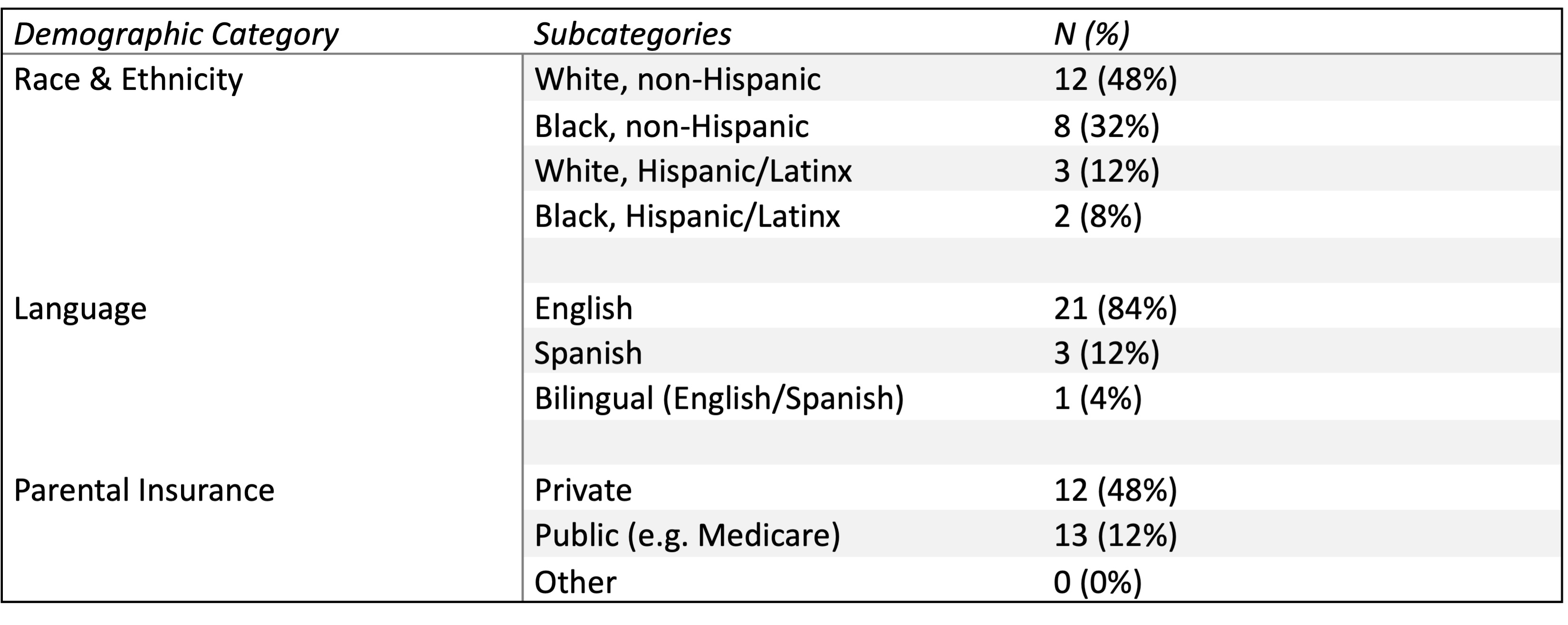
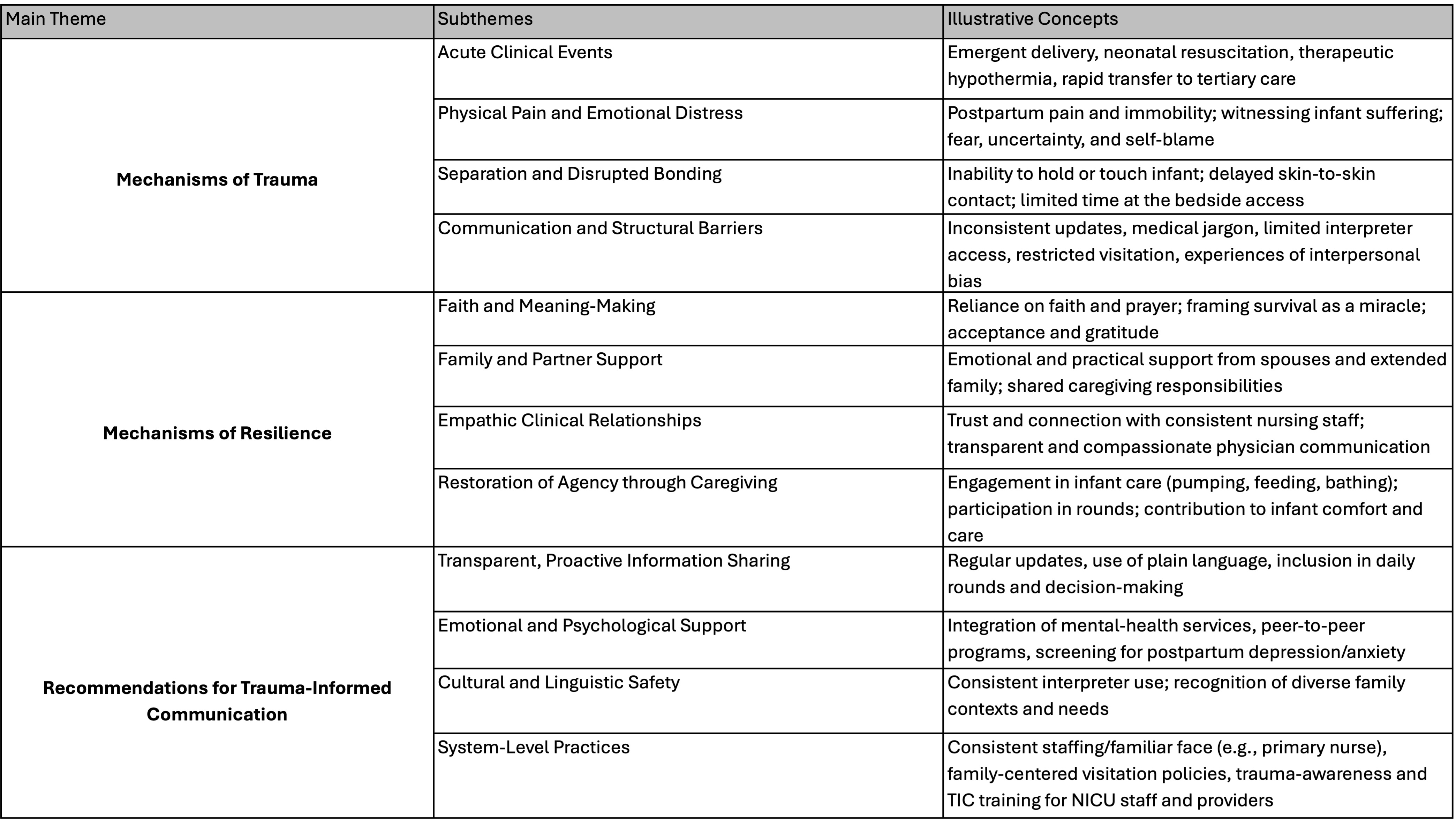
Background: Parents of infants with hypoxic-ischemic encephalopathy (HIE) often experience multifaceted trauma spanning pregnancy, birth, NICU hospitalization, and life after discharge marked by uncertainty about neurodevelopmental outcomes. Persistent communication gaps and limited integration of trauma-informed care (TIC) principles in NICU counseling contribute to parental distress. Understanding how trauma and resilience manifest across diverse sociocultural contexts is essential to improve care, communication, and equity in parental counseling and communication. Objective: To explore how parents of infants with HIE experience trauma and resilience during and after NICU hospitalization, and to identify opportunities for integrating trauma-informed communication into clinical practice. Design/Methods: Semi-structured interviews were conducted with former NICU parents (n = 22; 25 participants) whose infants (≥36 weeks GA) were treated for HIE at a tertiary medical center (2018-2024). Participants were purposively sampled for diversity in race/ethnicity, primary language, and insurance status. Interviews were transcribed, translated, and analyzed using the Sort and Sift, Think and Shift method, a qualitative research approach rooted in ground theory, constructivist, and phenomenology frameworks. Coding was iterative and guided by the six TIC principles: safety, trustworthiness, peer support, collaboration, empowerment, and cultural awareness. Results: Three main themes emerged: mechanisms of trauma, mechanisms of resilience, and recommendations for trauma-informed communication. Trauma mechanisms included acute perinatal events at delivery/birth, physical and emotional stress during the hospitalization, and separation/disrupted bonding. Emotional stress was compounded by inconsistent communication, language barriers, and experiences of bias. Resilience mechanisms centered on faith and religion, family support, and consistent, empathic nursing relationships. Active participation in care (pumping, feeding, bathing) restored parental agency and strengthened bonding. Recommendations emphasized proactive updates, inclusion during rounds, plain-language communication, consistent staffing, integrated mental-health support, and reliable interpreter access.
Conclusion(s): Trauma among NICU parents arises from both clinical and systemic factors, yet parents demonstrate resilience through faith, family connection, and engagement in their infant's care. Embedding trauma-informed principles, like emphasizing transparency, empathy, and inclusion, may mitigate secondary trauma and reinforce resilience, trauma-informed neonatal care.
Table 1. Parent/Caregiver Participant Demographic Information
Table 2: Themes and Sub-themes from Qualitative Analysis of Parental Experiences Following Neonatal HIE

 photo")