Session: Neo-Perinatal Health Care Delivery: Epidemiology/Health Services Research 4
57 - Does the evidence support the influence of low birthweight on adult health and disease in preterm infants? A systematic review of recent developmental origin studies
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4056.57
Shipra Jain, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Jacob Fry, Ohio University Heritage College of Osteopathic Medicine, Cincinnati, OH, United States; Sukanya Datta, University of Calgary, Calgary, AB, Canada; Tavleen A. Singh, Baptist memorial hospital - Desoto, Ms, Southaven, MS, United States; Seham Elmrayed, American University in Cairo, Calgary, AB, Canada; Tanis Fenton, University of Calgary, Calgary, AB, Canada
Dietitian/Epidemiologist/Professor University of Calgary Calgary, Alberta, Canada
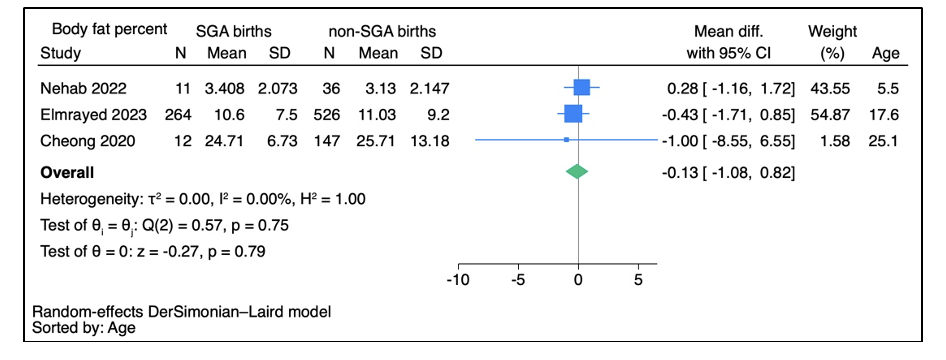
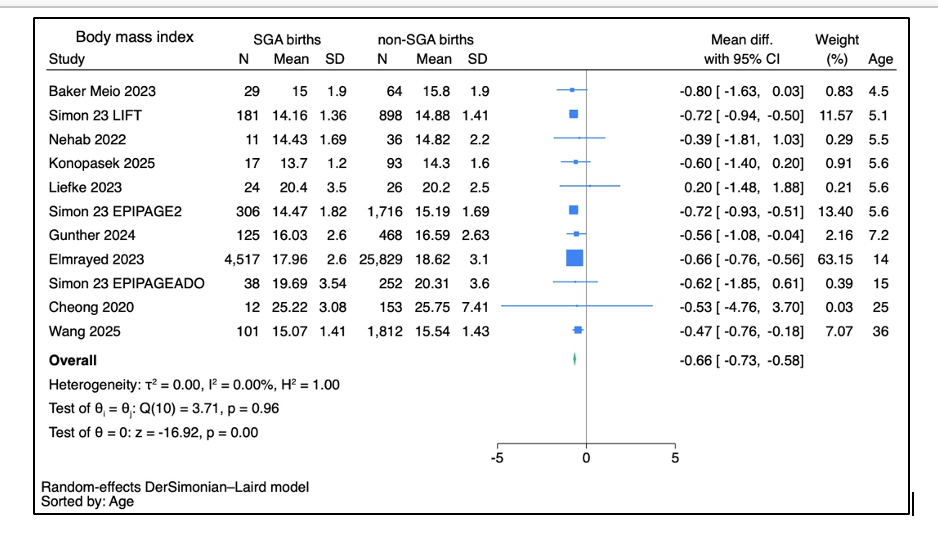
Background: The Developmental Origins of Health and Disease (DOHaD) hypothesis proposes that adverse intrauterine environments influence long-term cardiometabolic health. While low birthweight has been linked to later hypertension and metabolic syndrome, findings are inconsistent and often confounded by statistical overadjustment for later body weight or body mass index (BMI). Objective: To conduct a meta-analysis examining the association between small for gestational age birthweight in preterm infants and later cardiometabolic outcomes at ages >2 years and to evaluate whether associations differ by statistical adjustment for later weight or BMI. Design/Methods: MEDLINE and EMBASE were searched for studies published between January 2020 and June 2025. Eligible studies compared cardiometabolic or adiposity outcomes in preterm infants born small versus appropriate for gestational age. Screening and data extraction were performed in duplicate. Random-effects meta-analyses were conducted to generate pooled estimates, with subgroup analyses by adjustment for later weight/BMI. Results: Out of 4921 studies screened for titles and abstracts, 71 preterm infant studies were included for full text review, of which 16 studies met the inclusion criteria. None of the included studies adjusted for later weight or BMI. In later life, preterm SGA infants had a lower body mass index (-0.66 kg/m2, 95% CI −0.73, −0.58; 11 studies, I2 = 0%, n = 36,708, average age = 14 years, Figure 1), body fat (−0.13 kg, 95% CI −1.08, 0.92; 3 studies, I2 = 0.00%, n = 996, average age = 18 years, Figure 2), and systolic blood pressure (−1.29 mmHg, 95% CI −3.64, 1.05; 5 studies, I2 = 0%, n = 21,398, average age = 18 years, Figure 3).
Conclusion(s): Contrary to the DOHaD hypothesis, preterm infants born small for gestational age have lower adiposity and similar blood pressure and percent body fat in later life. The absence of increased cardiometabolic risk underscores the need for caution in restricting early nutrition among growth-restricted preterm infants and the importance of rigorous analytic approaches that avoid overadjustment bias.
Figure 1. Forest plot comparison: Later life body mass index for small for gestational age (SGA) versus non-SGA preterm infants
Figure 2. Forest plot comparison: Later life systolic blood pressure for SGA versus non-SGA preterm infants
Figure 3. Forest plot comparison: Later life body fat percentage for SGA versus non-SGA preterm infants


.png)