591 - Quality Improvement Focused Training for Pragmatic Implementation of Obesity Treatment in Primary Care
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4579.591
Jeremiah Salmon, American Academy of Pediatrics, Itasca, IL, United States; E. Jeanne Lindros, American Academy of Pediatrics, Itasca, IL, United States; Stephen R. Cook, Center for Healthy Weight & Nutrition / NCH, Columbus, OH, United States; Amanda E. Staiano, Pennington Biomedical Research Center, Baton Rouge, LA, United States; Sandra G. Hassink, American Academy of Pediatrics, Wilmington, DE, United States; Victoria Rogers, AAP, Saco, ME, United States; Denise Wilfley, Washington University in St. Louis School of Medicine, St Louis, MO, United States
Clinical Initiatives Manager, Institute for Healthy Childhood Weight American Academy of Pediatrics Itasca, Illinois, United States
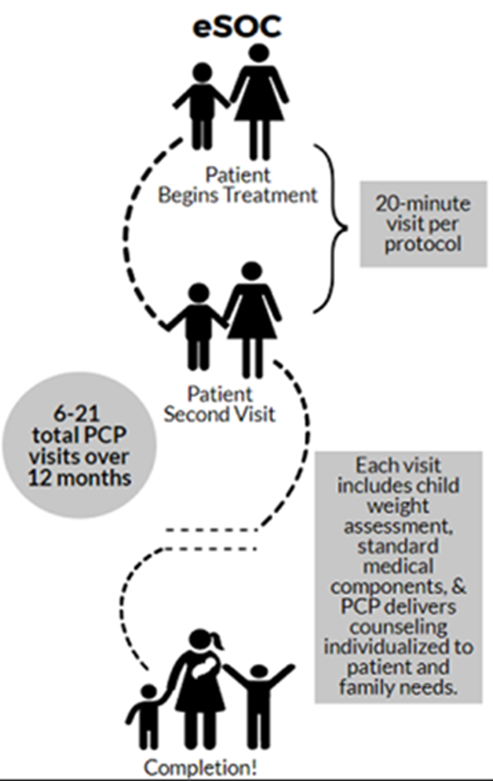
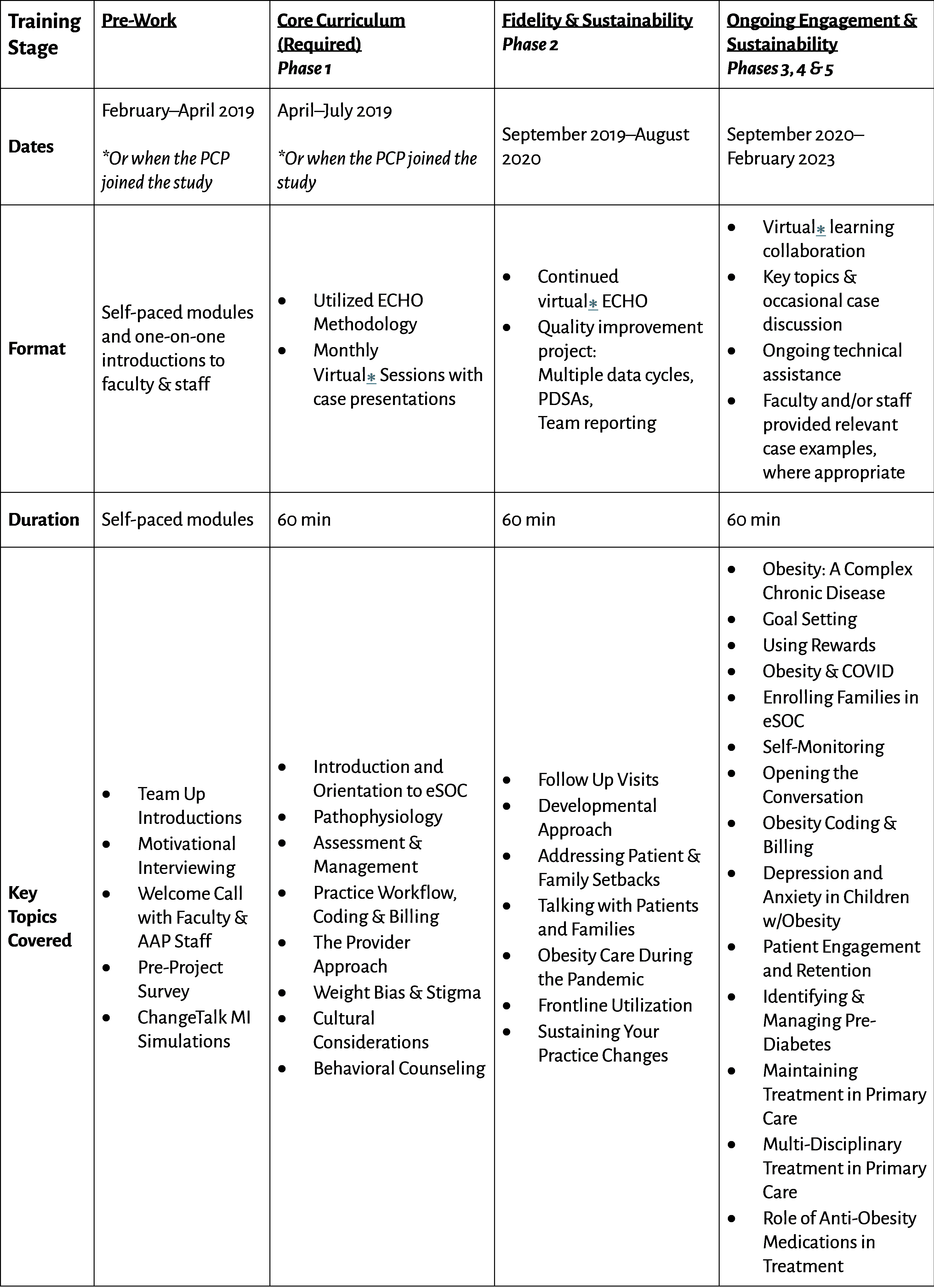
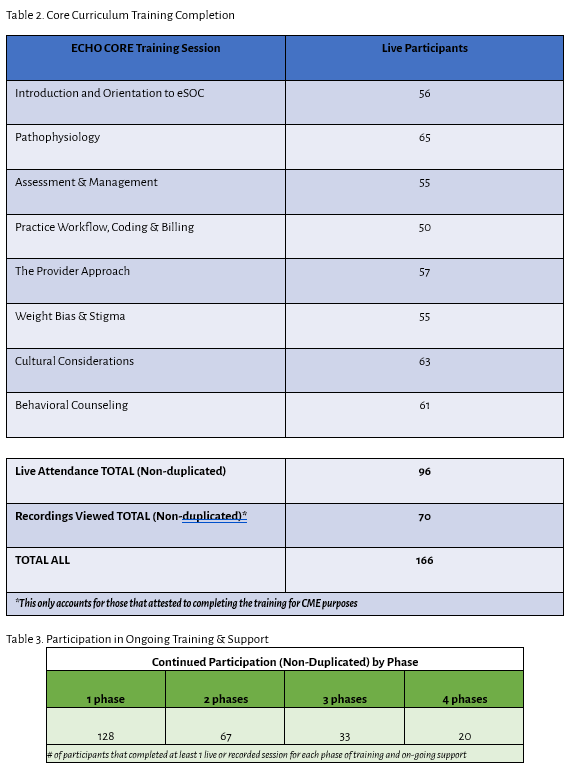
Background: Pediatric primary care providers were trained in delivering an enhanced standard of care (eSOC), (Fig 1), as part of a large pragmatic, comparative effectiveness trial (2019-2024), focused on obesity treatment. eSOC was compared with eSOC plus Family-Based Behavioral Treatment (eSOC+FBT), an evidence-based program delivering intensive health behavior and lifestyle treatment with trained interventionists. Previous studies suggest the important role that providers play in obesity treatment and potential for eSOC. Objective: Identify a pragmatic approach to addressing obesity in primary care. Design/Methods: To become a verified study provider, pediatricians and family medicine providers (MD/DO, NP/PA, etc.) completed eSOC Core Curriculum (Table 1), covering key topics such as medical management of obesity, behavioral counseling, and practical workflow considerations with a focus on implementation of national guideline concordant care. Once completed, providers/clinic teams were encouraged to join a virtual learning collaborative (VLC), which leveraged the ECHO model, combining didactic sessions and case-based learning. Later the VLC used the Model for Improvement framework, which uses 3 fundamental questions (i.e., what are we trying to accomplish, how will we know that a change is an improvement, and what change can we make that will result in improvement) along with plan-do-study-act (PDSA) cycles to drive practice change. In addition to QI activities and peer learning, Providers received a copy of Next Steps: A Practitioner's Guide of Themed Follow-up Visits to Help Patients Achieve a Healthy Weight. Results: The Core Curriculum was completed by 166 providers and clinical team members (Table 2). The ongoing training and VLC, broken into 4 phases (Table 3), had consistent participation throughout the intervention with 78% completing at least 1 additional phase beyond the initial required training, although provider engagement decreased over time. Providers reported changes to strategies they implement in practice (75%) and what they do in practice (80%). Reported changes included improved use of motivational interviewing, targeted comorbidity screening, monitoring labs more closely, and individualizing care among other changes based on the trainings and virtual learning collaborative.
Conclusion(s): Structured virtual eSOC trainings, virtual learning collaboratives, and peer learning can build clinical capacity and provider self-efficacy to deliver guideline concordant obesity care and ultimately increase access to evidence-based and effective obesity treatment in pediatric primary care obesity management.
Figure 1. eSOC Approach
Table 1. eSOC Core Curriculum and Ongoing Training
Tables 2 & 3. eSOC Core Training Completion and Ongoing Participation