334 - Outbound Transfers from Community Hospital's Neonatal Intensive Care Unit
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4327.334
Priyanka N. Arya, The Brooklyn Hospital Center, Brooklyn, NY, United States; Jade St. Paul, The Brooklyn Hospital Center, Brooklyn, NY, United States; Noah P. Kondamudi, The Brooklyn, Brooklyn, NY, United States
Resident Physician The Brooklyn Hospital Center Brooklyn, New York, United States
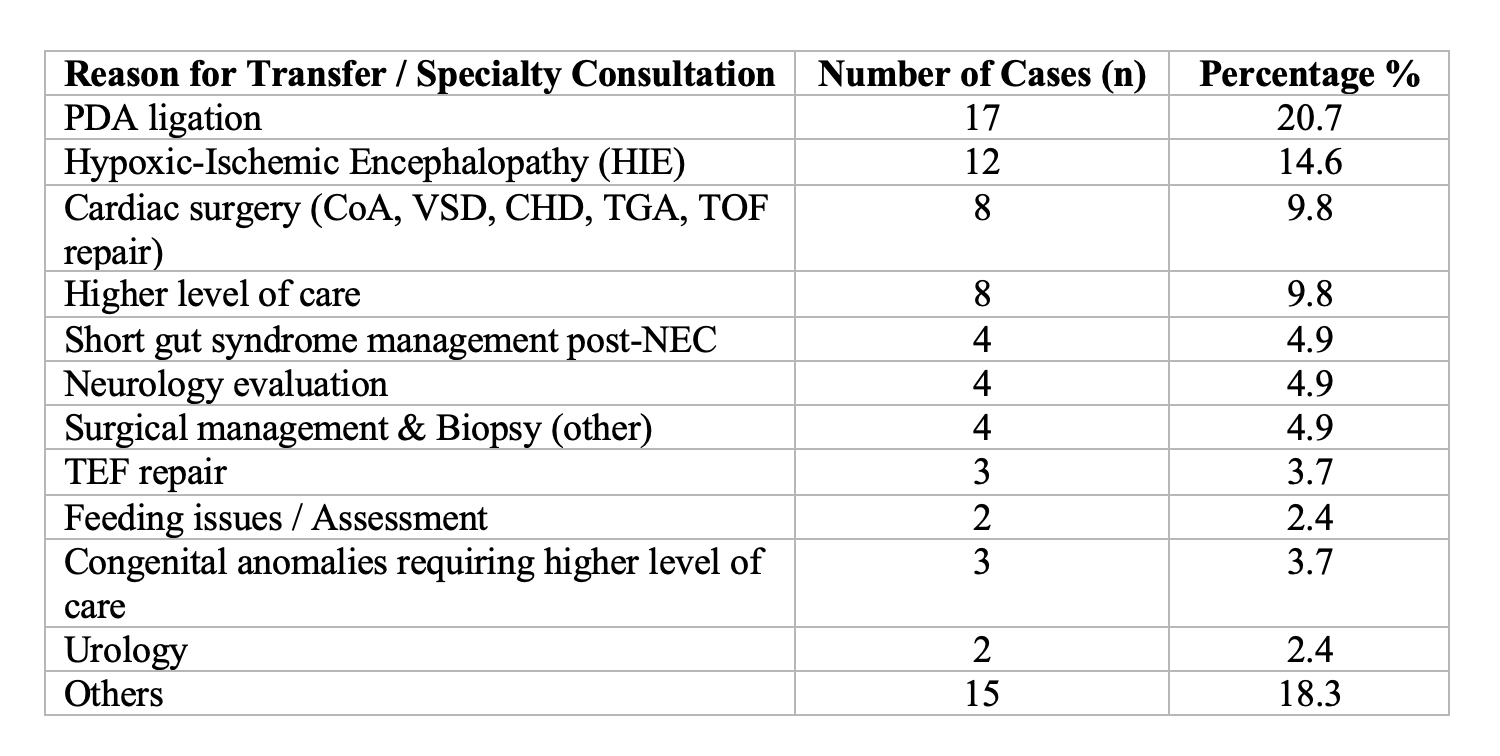
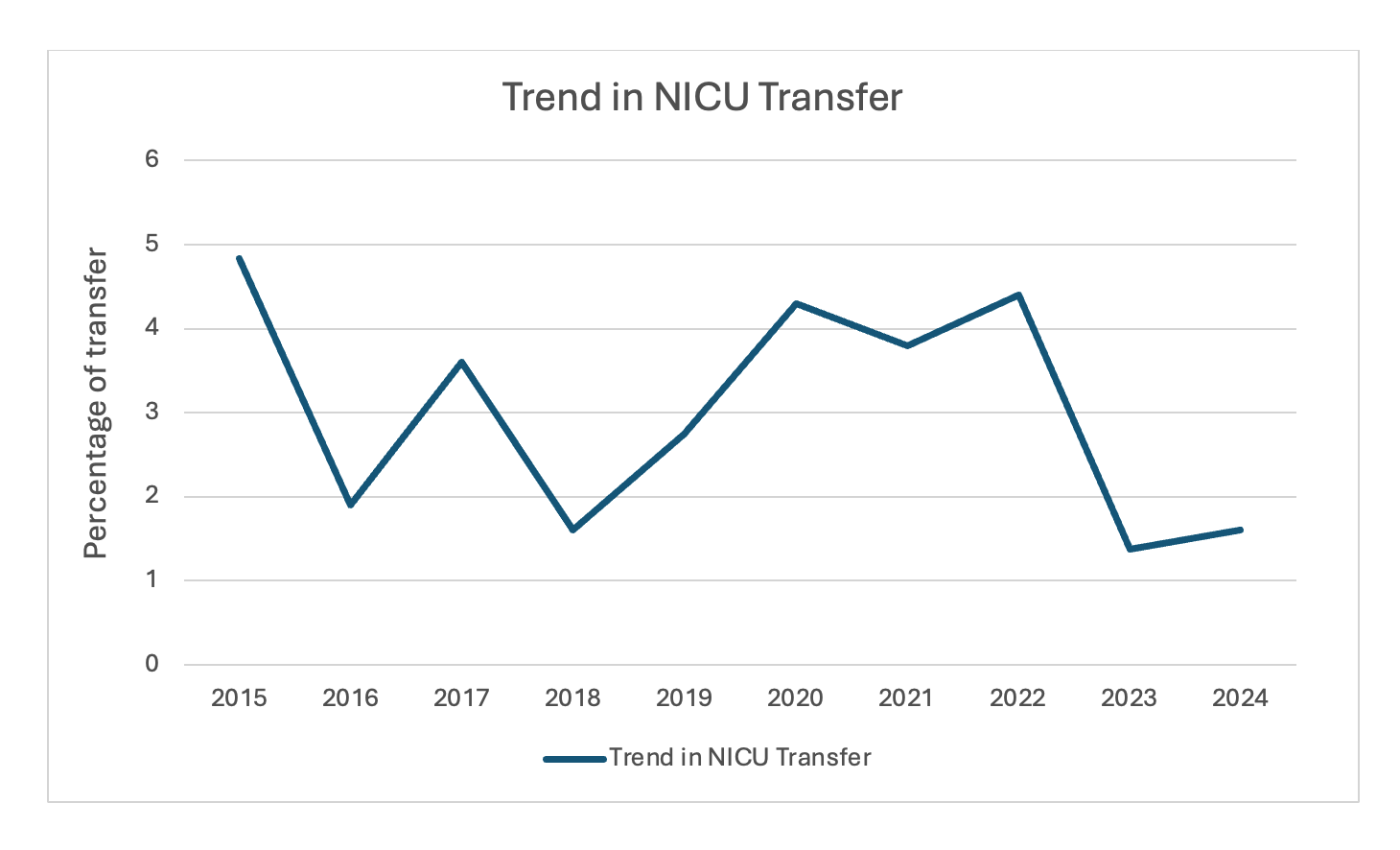
Background: Transfers from Level III Neonatal Intensive Care Units (NICUs) are typically necessitated by the need for advanced surgical or subspecialty care not available within community-based NICUs. Evaluating transfer patterns provides important insight into evolving neonatal care demands, supports quality improvement, and enhances regional collaboration among NICUs of varying levels. Objective: To analyze trends, clinical indications, and outcomes of neonatal transfers from a Level III NICU over a 10-year period at a community hospital. Design/Methods: A retrospective chart review of all neonates transferred from our Level III NICU between January 1, 2015, and December 31, 2024. Data obtained from NICU admission logs, transfer summaries, and electronic medical records. Variables collected included gestational age, birth weight, primary diagnosis, indication for transfer, destination hospital, and post-transfer outcome. Annual transfer rates were calculated as the number of transfers divided by total NICU admissions per year. Data were analysed using descriptive statistics, and temporal trends plotted in Microsoft Excel. Results: Of the 2,648 neonates admitted during the study period, 82 (3.1%) required transfer to a higher-level facility. The mean gestational age was 33 weeks (SD + 5.85) and the mean birth weight was 1,980 grams (SD + 1170). The most common indication for transfer was patent ductus arteriosus (PDA) ligation (n = 17, 20.7%) (Table 1). When categorized by systems, transfers related most often to cardiac (33%), neurologic (21%), and gastrointestinal (12%) systems. The highest transfer rate occurred in 2015 (4.8%), while the lowest noted in 2023 (1.8%) trending towards a gradual decline since 2022 (Figure). Seventeen infants (20.7%) subsequently transferred back to our NICU after completion of specialized interventions, indicating effective bidirectional coordination within the regional care network. Follow-up outcomes were available for 54 infants, of whom 53 (98%) survived.
Conclusion(s): Over the past decade, the rate of neonatal transfers to tertiary centers has shown a gradual decline since 2022 after peaks during the COVID and early COVID periods. This may be due to effective use of standardized transfer protocols, timely stabilization practices, and strengthened regional partnerships. PDA ligation, neurologic conditions, and complex cardiac were the leading reasons for transfer. The 20.7% transfer-back rate highlights effective coordination and continuity of care between community and tertiary NICUs.

 photo")