191 - Radiation exposure during O-arm surgical imaging at nine positions within the operating room
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3183.191
Eddie Geagea, Nemours Children's Hospital, Orlando, FL, United States; Mona Doshi, Nemours Children's Hospital, Orlando, FL, United States; John F. Lovejoy, Nemours Children's Hospital, Orlando, FL, United States
Research Fellow Nemours Children's Hospital Orlando, Florida, United States
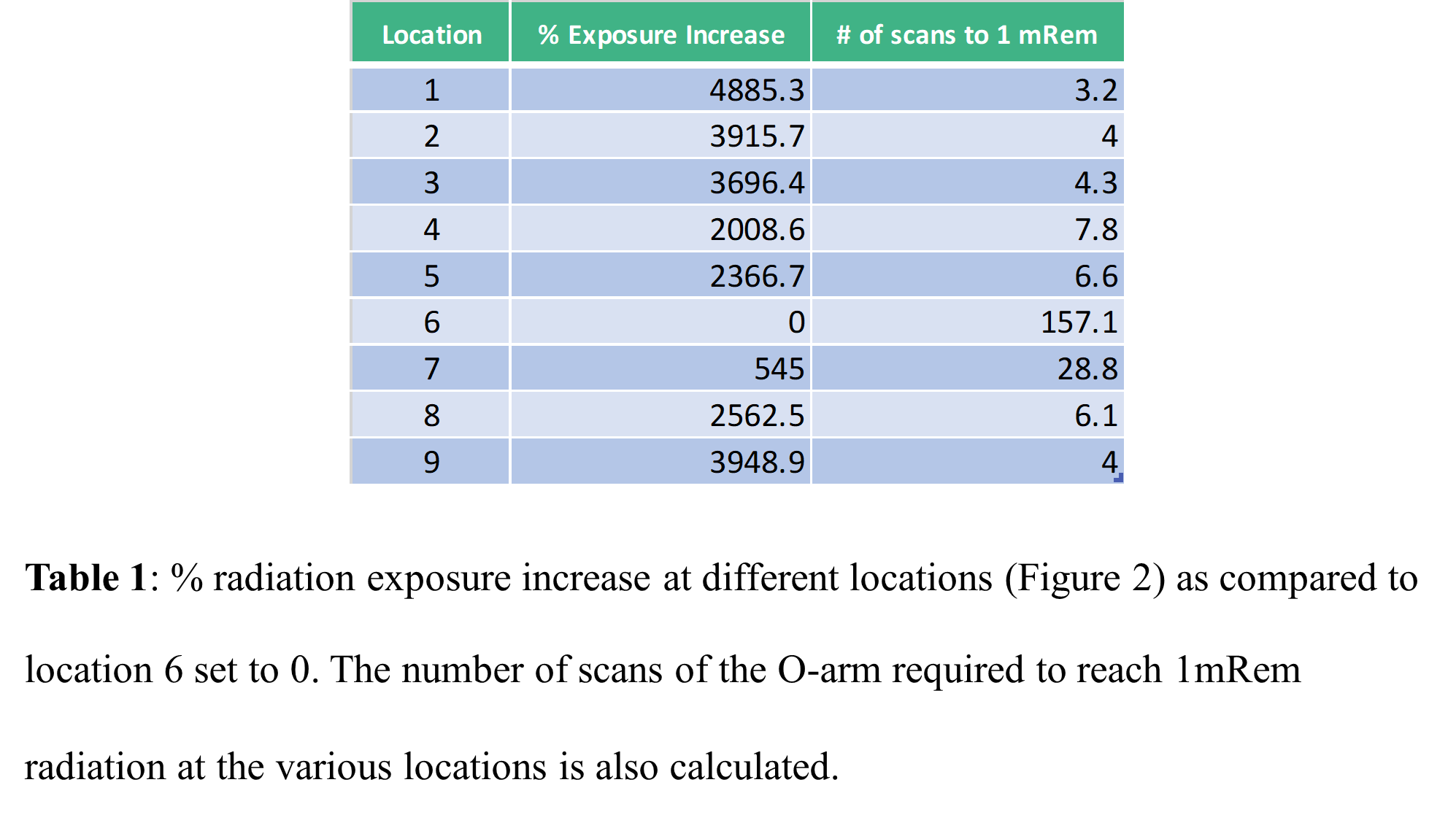
Background: The O-arm imaging system is widely used in spine surgery, enhancing surgical accuracy. However, it involves ionizing radiation exposure, which increases cancer risk for operating-room (OR) staff. The spatial complexity of scatter radiation, combined with variable staff positioning and imaging protocols, underscores the need for quantitative dose mapping. Objective: This article reviews patient characteristics, technical settings, and operator practices that influence O-arm-related radiation exposure and quantitatively assesses the dose with which OR personnel at multiple locations are exposed to during Pediatric Scoliosis Surgery. Design/Methods: A spine phantom, which mimics the patient being operated on, was used to evaluate radiation exposure during scan with the O-arm. We measured radiation exposure (µR) using a Victoreen Model 451P ion chamber positioned at 1.5 m (badge height) at nine locations each representing a designated area for OR personnel: 45° from phantom, nurse station, 15° from phantom, neuromonitoring, in front of lead wall, behind lead wall, behind control panel, anesthesiology, and behind far lead shield. The O-arm performed 360° rotations at low (10 mA, 40 mAs) and high (10 mA, 75 mAs) settings across several kVp values. Exposure was recorded for each location and setting. We calculated the percent exposure relative to the behind-lead-wall position and estimated the number of O-arm runs required to reach 1 mRem. Results: Personnel behind the lead wall received the lowest exposure, 6.2 µR, which is less than the background of 7 µR/hr. The highest exposure occurred at the anesthesiologist position, 184 µR, approximately 30-fold higher. Also, exposures increased progressively at unshielded positions closer to the O-arm.
Conclusion(s): Radiation exposure in the OR depends on personnel position; distance and lead shielding markedly reduce exposure. Reaching 1 mRem required approximately 5-160 runs depending on position. These values remain far below the annual occupational limits. Lead shielding and greater distance substantially reduce staff radiation exposure. Standing behind the lead wall yielded the lowest exposure, even below the background exposure, reinforcing safety protocols.

 Credit")
.png)