509 - Parental Acceptance of Nirsevimab for RSV Immunoprophylaxis: Single-Center Survey and Comprehensive Meta-Analysis
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3490.509
Julia Moniz Ganem, Yale School of Medicine, New Haven, CT, United States; Isabela Oliva, Yale School of Medicine, New Haven, CT, United States; Camila Aparicio Llorente, Yale School of Medicine, New Haven, CT, United States; Barbara Luiza R. Araujo, Yale School of Medicine, Department of Pediatrics, New Haven, CT, United States; Aanchal Wats, Yale School of Medicine, New Haven, CT, United States; Diego R. Hijano, St Jude Children's Research Hospital, Memphis, TN, United States; Carlos R. Oliveira, Yale School of Medicine, New Haven, CT, United States
Postdoctoral associate Yale School of Medicine New Haven, Connecticut, United States
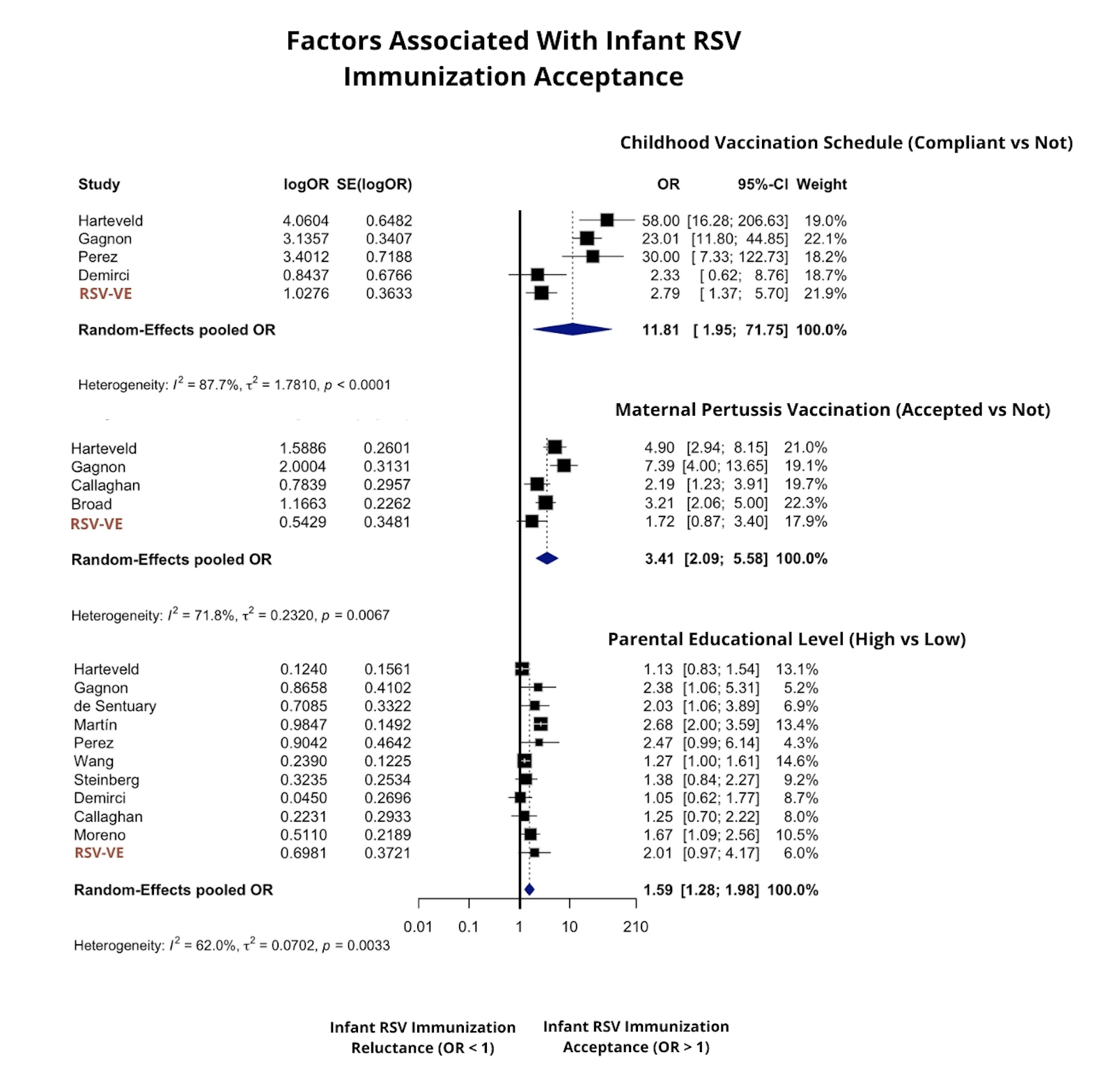
Background: Even highly effective public health interventions can fail to achieve population impact if uptake is low. Nirsevimab, approved in 2023, is the first-in-class long-acting monoclonal antibody for Respiratory Syncytial Virus (RSV) prevention in infants. Early data show wide variation in parental acceptance, ranging from 44% to 92%. Because nirsevimab is a monoclonal antibody rather than a vaccine, parents may not view it through the same lens as traditional immunizations. Objective: Examine how established vaccine-acceptance drivers extend to this class of interventions and identify key factors influencing caregiver decisions. Design/Methods: We used a hybrid cross-sectional and meta-analysis study design to integrate new caregiver survey data with global evidence on nirsevimab acceptance. Primary data came from the ongoing RSV effectiveness study (RSV-VE; NCT06172660), which enrolled Connecticut caregivers of infants eligible for nirsevimab in the 2024-2025 RSV season and assessed their attitudes and willingness to accept the intervention. In parallel, we performed a systematic review and meta-analysis following PRISMA guidelines. Literature databases were searched through September 2025 for observational studies examining perspectives toward nirsevimab (Figure 1). Pooled odds ratios (ORs) were estimated using random-effects models, heterogeneity was assessed with I² statistics, and study quality was evaluated using the NOS-XS2 scale. Results: A total of 172 caregivers completed the RSV-VE survey and were included in a meta-analysis with 21 additional studies (total n = 29,192; Figure 1). About 40% of RSV-VE participants were reluctant to accept nirsevimab (Table 1), compared with a pooled acceptance of 0.73 (95% CI: 0.66-0.80) across studies. To contextualize these findings, we examined predictors of caregiver receptivity. Prior vaccination behavior was the strongest factor (Figure 2): caregivers adhering to childhood schedules were more likely to accept RSV immunization (OR = 11.81, 95% CI: 1.95-71.75). Maternal acceptance of prenatal pertussis vaccination also positively correlated with infant RSV immunization willingness (OR = 3.41, 95% CI: 1.67-6.97), with country-level subgrouping explaining heterogeneity. Higher parental education was likewise associated with nirsevimab acceptance (OR = 1.59, 95% CI: 1.27-2.00; Figure 2).
Conclusion(s): Established determinants of vaccine acceptance appear to extend to nirsevimab. Prior vaccination behaviors were the strongest predictors, emphasizing the potential of coordinated pediatric and maternal vaccination strategies to improve acceptance.


.jpg)