Vice chair | Department of Neonatology Cleveland Cleveland, Ohio, United States
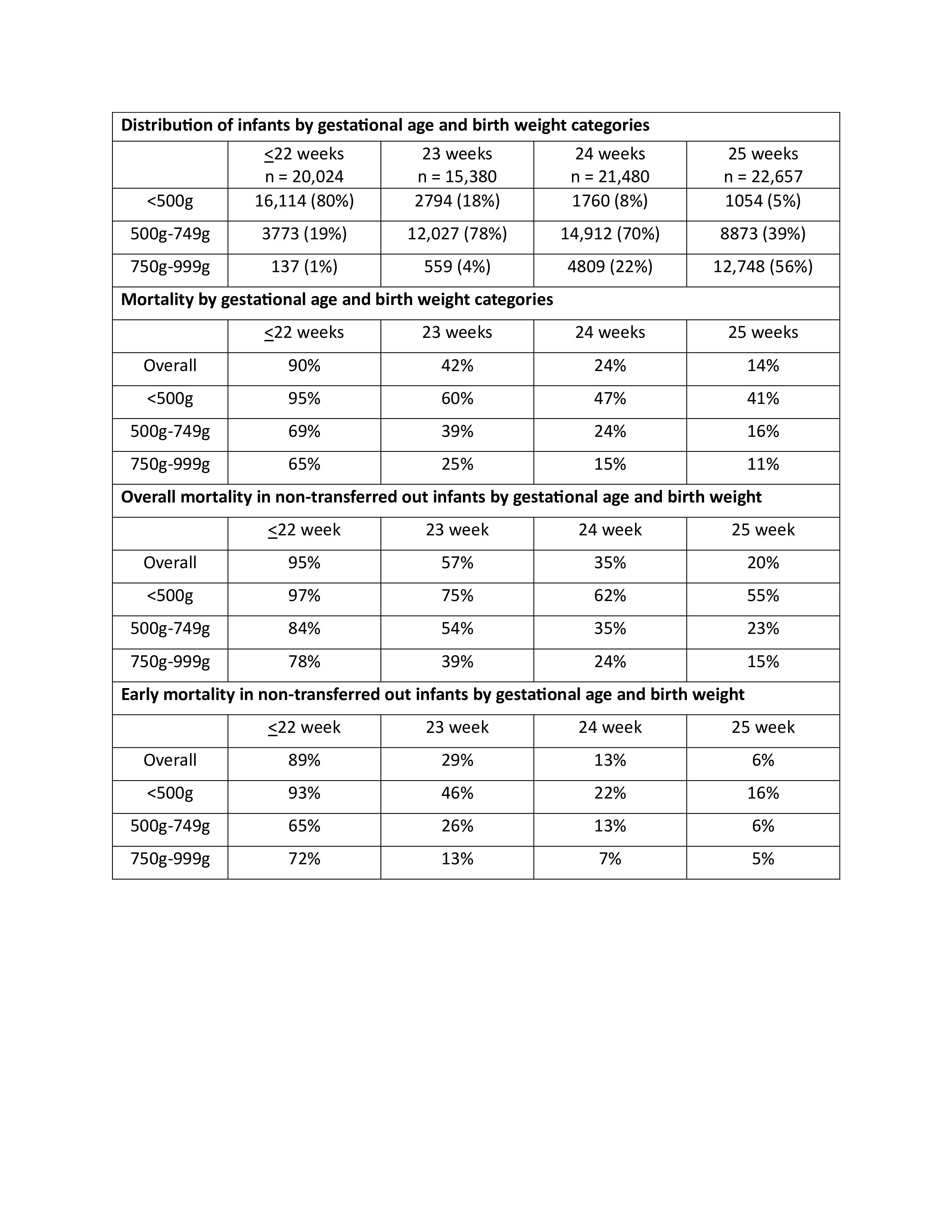
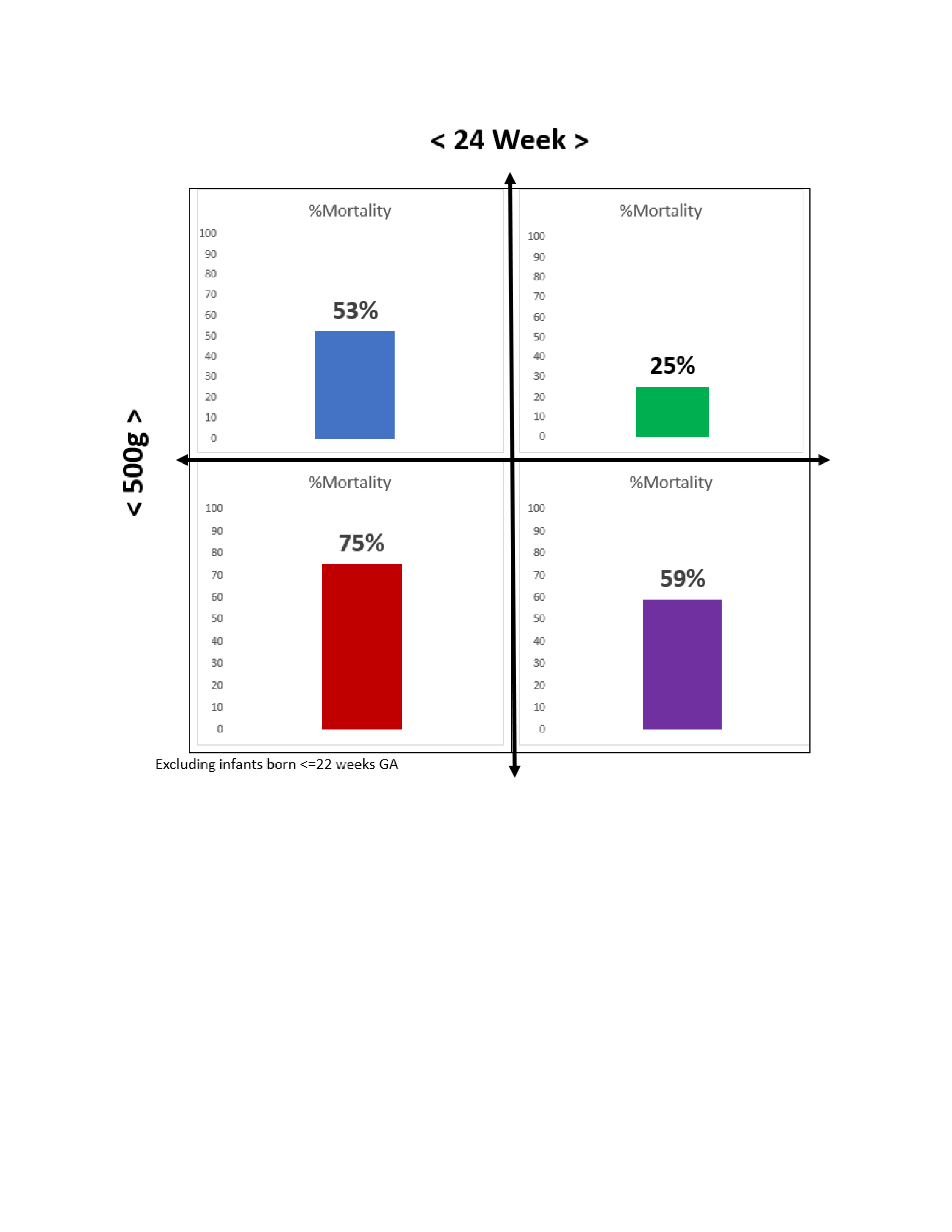
Background: Earlier reports highlighted gestational age (GA) as a favorable predictor of survival compared to birth weight (BW) in infants at the edge of viability. It is not clear if this assumption is still valid with the evolving practice of resuscitating extremely immature infants. Objective: To examine whether GA or BW is more impactful on the survival of extremely low birth weight (ELBW) infants born at ≤25 weeks GA. Design/Methods: We used the datasets produced by the Healthcare Costs and Utilization Project (HCUP) for the years 2016-2022. We included infants ≤25 weeks GA and < 1000g BW. We excluded infants diagnosed with congenital and chromosomal anomalies. The frequencies of infants delivered at each combination of GA (≤22wk, 23wk, 24wk, and 25wk) and BW ( < 500g, 500-749g, and 750-999g) were calculated. In addition, mortality within the first 24h and overall mortality were calculated. Results: The study included 79,560 infants. Majority of infants ≤22wk GA (infants born at 22wk and 21wk) were in the < 500g BW category. Majority of infants born at 23wk and 24wk GA were in the 500g-749g BW category, while infants 25wk GA were split between 500g-749g and 750g-999g BW categories. Infants transferred out of the delivery hospital were 23%, and overall mortality was 41%. Transfer out was limited to 5% in ≤22wk infants while mortality was 90% (95% if non-transferred) reflecting failure of resuscitation efforts with early mortality or a decision not to resuscitate. Less than 1/3 of infants 23-25 weeks were transferred out with mortality declining from 42% in 23wk infants to 14% in 25wk infants. Majority of infants in the ≤22wk GA category expired regardless of the BW. Although declining with advanced GA, majority of infants in the < 500g BW category expired regardless of the GA; 95% in ≤22wk GA and 55% in 25wk infants. Excluding infants ≤22wk, mortality in infants < 24wk and < 500g was much higher than infants ≥ 24wk and ≥ 500g, 75% vs. 25%, OR 8.9 (CI:8.1-9.9), p < 0.001. On the contrary of previous reports, infants < 24wk but => 500g had less mortality compared to infants ≥ 24wk but < 500g, 53% vs. 59%, OR 0.08 (CI:0.71-0.86), p < 0.001.
Conclusion(s): Despite recent advances in neonatal resuscitation, more than 95% of infants born at ≤22wk expire, mostly in the first day of life. In addition, most infants < 500g expires (97% in ≤22wk down to 55% in 25wk). BW ≥ 500g may be associated with better mortality outcome compared to GA in infants at the edge of viability.