351 - Dexamethasone therapy for Bronchopulmonary Dysplasia in a level III NICU
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2340.351
Troy Davidson, University of Tennessee Health Science Center College of Medicine, Memphis, TN, United States; Ajay J. Talati, University of Tennessee Health Science Center College of Medicine, Memphis, TN, United States; Andrew Mire, University of Tennessee Health Science Center College of Medicine, Memphis, TN, United States
Resident University of Tennessee Health Science Center College of Medicine Memphis, Tennessee, United States
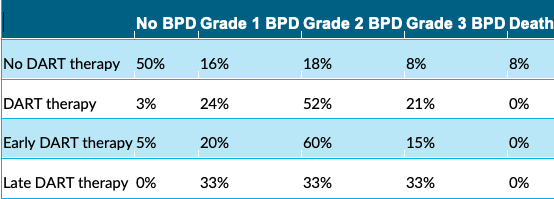
Background: There has been widespread research of corticosteroids in the management of Bronchopulmonary Dysplasia (BPD). Further investigation is needed to evaluate efficacy in neonates. Information about the risks and benefits is useful when making the decision to start. The 2022 NICHD Neonatal BPD Outcome Estimator is an online tool available to help quantify risk of BPD. Objective: Our objective is to analyze data from our level III NICU by investigating if correlation exists between the timing of steroid initiation and respiratory status at 36 weeks PMA, as well as how applicable the calculator was to our population. Design/Methods: In our retrospective cohort study, we included neonates admitted to our Level III NICU from 1/4/2024-6/24/2025 with a gestational age less than 29 weeks. NICHD Neonatal BPD Outcome Estimator retrospectively stratified risk for BPD at 14 and 28 days of life based on respiratory settings, birth weight, and gestational age. With an unpaired t test, we compared the risk stratification for patients who started the suggested 10 days of DART therapy prior to DOL 28, to that of the remainder of the cohort. Patients were then evaluated at 36 weeks PMA on BPD status, with or without DART using chi squared analysis. Early DART therapy outcomes (started < 28 DOL) were compared to late therapy outcomes. Results: There were 84 neonates pertinent to our study, 82 born at our unit. 48 neonates were male. The range of gestational ages was 22.0 to 28.6 (Mean 26.1, Median 26.2). The average birthweight was 795 grams (Range 420-1220, Median: 780 grams). All received caffeine within 24 hours of life. 72 received surfactant within two hours. None started DART therapy prior to DOL 14. Non-DART recipients had a lower risk of BPD at 36 weeks PMA than those who did (p < 0.05). No subject in the steroid group died. The steroid group had a higher rate of Grade II BPD (p < 0.05). Early DART versus late showed no significance at 36 weeks PMA. Using the NICHD calculator, our t test showed significant risks for Grade III, II, and "no BPD" at DOL 28 when comparing the steroid to the no steroid group.
Conclusion(s): While this study did not factor in all comorbidities, it associates DART therapy with higher rates of Grade II BPD and lower rates of "no BPD". The severity of lung disease and duration of mechanical ventilation prior to dexamethasone initiation were not evaluated. The NICHD calculator overall underestimated Grade III BPD and overestimated Grade I in our population. A larger sample size is required. DART therapy should be used with caution in neonates, and warrants further investigation in a prospective study.
BPD outcomes at 36 weeks corrected gestational age

 photo")